
IMPORTANT
Age-related macular degeneration can be effectively treated with new therapies known as intravitreal injections. The two main therapies are Lucentis and Avastin. However the success of these treatments can depend on how soon the disease is detected. It is imperative that if you have any of the symptoms listed below, and you are in the "at risk" age group, that you have your eyes checked. If you are a private patient, Niall Patton can organise this for you promptly and carry out your injection treatment as soon as possible. Otherwise, your optometrist can provide you with useful advice and you may need to attend your local NHS ophthalmic service promptly.WHAT IS IT?
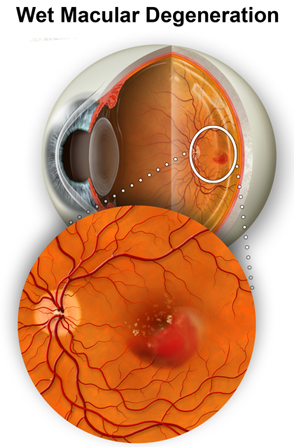
As its name suggests, age-related macular degeneration (ARMD) is degeneration of the center part of the retina (called the macula) that occurs as some individuals get older. The retina acts like the film in a camera, and good anatomical function of the retina is vital for good vision. Indeed, the most important part of the retina is the macula, as that is the part of the retina that provides our high-level central vision that we use for things such as reading, watching television, recognising faces, etc. If ARMD develops, the macula degenerates, and loses good function. As a result, the vision is very poor. ARMD is so common that it is the number one cause for visual impairment and resulting blind registrations in Western countries. The cause for ARMD is unknown, but factors that are known to play a part include age, genetics (more common in those that have a family history), smoking, and other environmental factors such as diet may also play a role. There are two main types of macular degeneration, commonly referred to as dry age-related macular degeneration and wet age-related macular degeneration.

Dry Age-related Macular Degeneration is the most common form of the disease, accounting for approximately 90% of cases. Dry ARMD develops more slowly than wet ARMD, but can progress to result in significant loss of central vision. There are no treatments as such for dry ARMD, though patients should be warned about the risk of developing distortion and sudden loss of central vision, as this can be the herald of newly developing wet ARMD. Magnifying lenses may offer some help in the patient managing activities of daily living.
Wet Age-Related Macular Degeneration only accounts for approximately 10% of cases, but the results can be devastating to the vision. It is usually as a result of "new" blood vessels growing under the retina. These blood vessels displace and damge the overlying retina, and in addition can bleed and scar resulting in loss of vision.
WHO GETS IT?
As stated above, no "cause" as such has been identified for ARMD. However, there are several groups that are known to be at higher risk than others in the likelihood of developing the disease:the elderly, those with a family history, and smokers.
WHAT ARE THE SYMPTOMS?
For those with early disease, there may be little in the way of symptoms, and the disease may only be recognised by your ophthalmologist inspecting the retina as part of an ophthalmic examination. However, as the disease progresses, symptoms of central distortion (so-called metamorphopsia, see diagram above) and loss of central vision occur. It is very unusual for ARMD to affect the peripheral vision. Thus, even in end-stage disease, few patients end up with complete blindness, though they are severely incapacitated by loss of their central vision, resulting in them being unable to read, watch television or recognise faces without great great difficulty.

Amsler Grid
HOW IS IT TREATED?
Until recently, there were very few effective treatments for ARMD, and even today there are signifcant limitations on current therapy, for example no treatment is currently available to treat dry ARMD. However, in the past few years, an array of exciting new treatments known as anti-VEGF therapies have become available and these have transformed the management of wet ARMD. These treatments may not only stabilise the vision due to wet ARMD, they may also improve it in certain patients. There are significant drawbacks to the treatment however, not least the fact that the treatment consists of injections into the eye (usually repeated every month for at least three months and often more). These anti-VEGF therapies include Avastin, Lucentis and Macugen. An additional concern is the cost of these new therapies and the ability of the NHS to fund them. Currently, at Manchester Royal Eye Hospital, a new comparative trial (GMAN) of different "Avastin" regimes is underway for patients with "wet" ARMD. It is important to remember that although the new therapies are a major advance on previous treatment, there are still certain individuals with wet ARMD for whom therapy is not indicated.

For further information regarding treatment of Age-related Macular Degeneration, Niall Patton has developed a website dedicated to information on this: www.eye-injections.com